
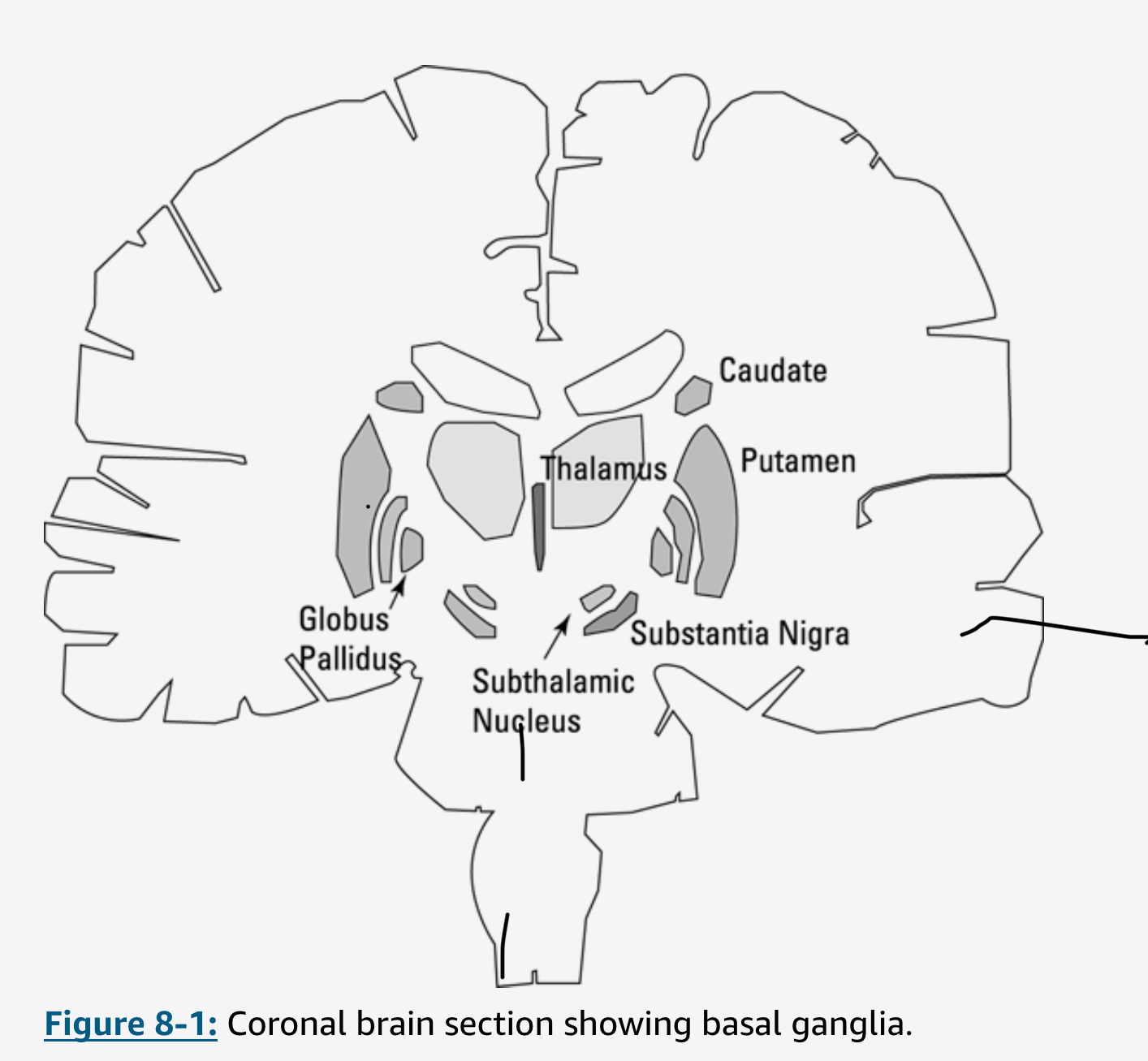
Parkinson’s Disease (PD) is an idiopathic, neuro-degenerative condition related to the loss of function of specialized cells in the lower mid-brain which stimulate the production of the neurotransmitter dopamine, specifically in the substantia nigra (SN), which is part of the basal ganglia (see illustration below). As much as 60% of its dopamine receptors are usually lost before diagnosis, starved to death, as it were.
Among the symptoms are disruptions in gait, the “senior shuffle”, freezing of steps, as well as festination, a hurrying pace aggravated by stooping and loss of balance which can provoke falls. Also symptomatic of PD are facial-masking (hypomimia) and micrographia (altered handwriting), hypophonia (weakened voice)), bradykinesia (slow movements), tremors, rigidity, and a general lapse of dexterity.
Many neurons in the cortex of the brain send axons down the spinal cord and synapse on the alpha or principal motor neurons that innervate muscle fiber. This spinal pathway, called the pyramidal system, provides fine control of muscles all the way to the toes but, significantly, to the hands and fingers..
Normally, the dopamine released in the SN amplifies activity in this direct circuit, supporting cortical activation of movement. Reduction of dopamine in the SN accordingly results in a lessening of “higher” direct cortical control of muscles. Hence the loss of dexterity
The brain is an electrical-chemical machine exhibiting a kind of yin/yang balance of positive and negative charges, which are usually described as excitatory and inhibitory in nature. There are billions of neurons and neuronal links or synapses in the brain and they are densely interconnected. So alongside and in parallel with the direct pathway between the cortex and the muscle nerves there are indirect pathways between the SN and the thalamus, which itself regulates, in coordination with various areas in the neo-cortex, motives, goals and movements. This is called the extrapyramidal system because it runs besides the pyramid-shaped neurons in the neo-cortex.
Dopamine released by the SN reduces the effect of this indirect extrapyramidal control. It follows that any decrease of dopamine increases inhibition along this pathway. This doesn’t exactly equate with dysfunction, since there are a gazillion variables at play in each and every brain. But it does negatively impact planned, programmed and intended movement.
Dopamine also is important in regulating the frequency of brain waves, in particular in the basal ganglia and subthalamic regions which are important for the preparation of voluntary movements. Different frequency bands have different names, such as beta for 15 Hz to 30 Hz and theta for 3 Hz to 10 Hz. Synchronization of subthalamic nucleus activity in the beta band is associated with movement initiation.
Deficiency of dopamine interferes with the ability to initiate and execute selected movements and also sets off the abnormally large, static, synchronized rhythms associated with PD’s limb tremor (sometimes mistaken for “essential tremor”). Composite medications like carbida-levadopa, the carbida acting as a kind of bodyguard escorting the levadopa across the brain-blood barrier, affect these persistent beta oscillations and kick them above 60 Hz up to the high-gamma band, calming the physical symptom of inner disorder of PD, once named the “shaking palsy”. Traditional Chinese and Sanskritic medicine had names of their own for this disease.
Though the symptoms of PD can be abatted by pharmaceuticals, especially levadopa, the progess of the disease is inexorable. Moreover, the efficacy of dopamine surrogates like levadopa unfortunately wears out over time. There are some non-pharmaceutical options, including Deep Brain Stimulation (DBS). This consists of inserting a probe into the subthamalmic nucleui down to the SN, then applying electrical charges, much like a pacemaker. DBS has relieved the symptom in thousands of PWPs without the side effects that occur with pharmaceutical therapies.
Yet PD remains a mysterious disease. There is no cure.
Obviously, I haven’t chosen to write this piece for serendipitous reasons. See Diagnosis for an earlier take on my affliction.
Readings / Sources:
Amthor, F. 2020. Neurobiology For Dummies. Hoboken: John Wiley & Sons. Notes: https://alteritas.net/alteritas/2024/01/28/notes-to-neurobiology-for-dummies/
——–. 2023. Neuroscience for Dummies. 3rd Edition. Hoboken: John Wiley & Sons. Note: https://alteritas.net/alteritas/2024/01/28/notes-to-neuroscience-for-dummies/
Austin, James H. 2006. Zen-Brain Reflections: Reviewing Recent Developments in Meditation and States of Consciousness. MIT Press.
Godfrey-Smith, Peter. 2016. Other Minds: The Octopus, the Sea, and the Deep Origins of Consciousness. Farrar, Straus and Giroux.. Notes: https://alteritas.net/alteritas/2023/12/25/highlights-from-other-minds/
Presti, David E. 2015. Foundational Concepts in Neuroscience: A Brain-Mind Odyssey (Norton Series on Interpersonal Neurobiology). Notes: https://alteritas.net/alteritas/2023/12/24/highlight-notes-from/
Sapolsky, Robert M. 2017. Behave: The Biology of Humans at Our Best and Worst. Penguin Publishing Group. Notes: https://alteritas.net/alteritas/2024/01/19/highlights-and-notes-on-behave-the-biology-of-humans-at-our-best-and-worst-by-sapolsky-robert-m/
Thaler, Alison I., and Malcolm S. Thaler. 2021. The Only Neurology Book You’ll Ever Need. Wolters Kluwer Health, 2021. Notes : https://alteritas.net/alteritas/2023/12/24/highlight-notes-from-neurology-readings/